Author: Julie Sufana


contextflow winner of the Healthy Hub competition from four health insurance companies: Innovative solutions for women’s health and early detection
DORTMUND, 13.03.2024. The winners of the 2024 Healthy Hub Competition want to improve women’s health with innovative care. The various offers relate to different phases of life and clinical pictures – from hybrid tests against HPV viruses, to care for typical female diseases such as endometriosis, to innovative therapy for menopausal symptoms. People with lung diseases should receive better care in terms of early detection. The winning teams will each tackle these topics with one of the four health insurance companies – BIG direkt gesund, IKK Südwest, mhplus Krankenkasse and SBK Siemens-Betriebskrankenkasse. This is the fifth time that the health insurance companies have jointly organized the competition.
“This time, the focus was on selected contractual care solutions, which take into account the gender health gap, i.e. the inequality of care between women and men,” explains Dr. Elmar Waldschmitt, Managing Director of the Healthy Hub and Board Representative at BIG. Unfortunately, medical research and care is still too heavily focused on men.
The winners were selected from over 40 applications:
Remi Health, health insurance partner BIG direkt gesund
Remi Health has developed a cervical cancer screening program that allows insured women to test themselves for human papillomavirus (HPV) at home. If the results are positive, an online consultation and an appointment with a gynecologist are provided. Remi’s digital platform also provides information about the importance of screening and early detection. “The low-threshold HPV test combines home testing, telemedicine and prevention in one seamless process,” explains Marvin Abert, Co-CEO of Remi Health. “In particular, we want to reach young women who have not yet taken advantage of cancer screening and have no immunity through an HPV vaccination. In our opinion, the HPV self-test from Remi Health is an innovative approach to complementing cancer screening in a meaningful way,” says Christiane Heidrich, Team Leader Managed Care at BIG direkt gesund.
Femna Health, health insurance partner SBK Siemens-Betriebskrankenkasse
Around a third of women of fertile age, i.e. in their fertile years, suffer from severely restrictive physical, psychological and social stress due to cycle complaints. These include conditions such as PMS, endometriosis and dysmenorrhea. “Current care does not adequately address these problems due to a lack of treatment options, long waiting times and a lack of individualized care. FEMNA has therefore developed a hybrid care model that provides women with improved, comprehensive and immediate care,” explains Maxie Matthiessen, founder of Femna Health. “Femna Care improves behavioral patterns and helps to prevent secondary diseases and increase the quality of life of affected women,” says Christina Bernards, Team Leader Care Management, SBK Siemens-Betriebskrankenkasse. “This is an issue close to our hearts, because women’s health in particular is massively neglected and underfunded in medicine and research. It’s time we changed that.”
YoniCare, health insurance partner mhplus Krankenkasse
With YoniCare (MICADO HEALTH CARE GmbH), the Healthy Hub has a non-digital care product in its portfolio for the first time. YoniCare enables laser therapy for the treatment of genitourinary syndrome. “The drop in estrogen levels during the menopause leads to vaginal dryness, changes in vaginal tissue and the vaginal mucosa and, as a result, symptoms such as itching, incontinence, infections and other complaints,” says Mandy Wilms from MICADO HEALTH CARE GmbH. The therapy can revitalize the vaginal epithelium that lines the vagina and the vaginal vestibule. The symptoms decrease and gynecological health is restored. “The therapy can make hormone replacement therapy superfluous and reduce interactions with medication,” says Fabienne Knaub, consultant for selective contracts and care analysis at mhplus Krankenkasse.
contextflow, health insurance partner IKK Südwest
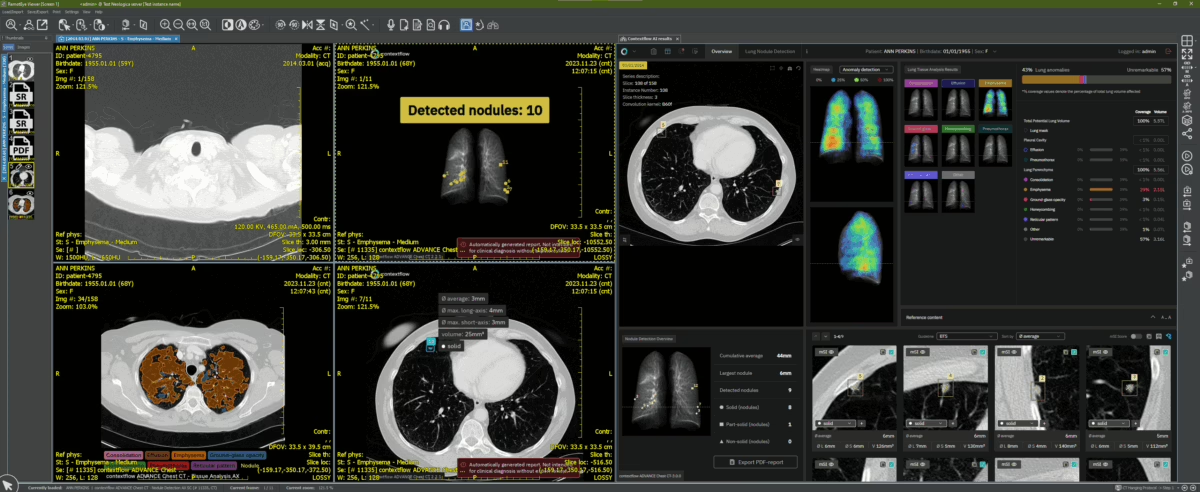
Early detection is essential for successful treatment of thoracic diseases. “We offer AI software that provides additional information for identifying and interpreting lung-specific image patterns in CT scans,” says Markus Holzer, CEO and co-founder of contextflow. The ultimate goal of the software is to detect lung cancer as early as possible in order to save healthcare system resources and protect patients from unnecessary interventions. “The image analysis AI enables radiologists to assess relevant image patterns of lung cancer and respiratory diseases faster and better,” says Dr. Florian Brandt, Health Innovation Manager at IKK Südwest.
Developing use cases for healthcare practice
Over the next few months, the four health insurance companies will work with the winning teams to develop specific use cases that are suitable for use in statutory health insurance (SHI). “Our aim is to ensure that these innovative care methods are used in practice,” says Dr. Elmar Waldschmitt. In addition, the Healthyhub’s cooperation partner, GWQ ServicePlus AG, will be involved in the development from the outset.
About the Healthy Hub
Since 2018, the four health insurance companies BIG direkt gesund, IKK Südwest, mhplus Krankenkasse and SBK Siemens-Betriebskrankenkasse have been committed to the digitalization of the healthcare system with the Healthy Hub. The aim is to enable innovative solutions for better, integrated care. To this end, the health insurance funds regularly organize competitions for start-ups. They have already brought 27 start-ups into the healthcare sector.
About BIG direkt gesund
BundesInnungskrankenkasse Gesundheit – BIG direkt gesund for short – was founded in Dortmund in 1996. The big idea behind BIG: We create space for being human. This means a modern online approach and empathetic service that is fast and solution-oriented. BIG offers versatile communication channels to suit the respective lifestyles of its around 510,000 policyholders across Germany. These customers receive appreciative and understandable advice by phone, chat, email or letter. Many additional benefits and an attractive bonus program are further major plus points. BIG direkt gesund has its legal domicile in Berlin, its head office in Dortmund and an important administrative location in Aachen. BIG employs around 950 staff at its operating locations and offers on-site advice in 11 BIGshops.
For inquiries
Bettina Kiwitt
Head of Corporate Communications
Phone: 0231/5557-1016
E-mail: bettina.kiwitt@big-direkt.de
About IKK Südwest:
IKK Südwest currently serves more than 635,000 insured persons and over 90,000 companies in Hesse, Rhineland-Palatinate and Saarland. Insured and interested parties can rely on personal support in our 21 customer centers in the region. In addition, IKK Südwest can be contacted around the clock seven days a week via the IKK service hotline 0681/ 3876 1000 or at www.ikk-suedwest.de.
For inquiries
Mathias Gessner
Press spokesman
Phone: 0681/3876-1163
E-mail: presse@ikk-sw.de
About the mhplus health insurance company:
mhplus Krankenkasse is open to those with statutory health insurance. Around 1,000 employees look after more than half a million policyholders throughout Germany. Independent tests confirm high service standards and solid finances. The mhplus supplementary contribution has remained stable at 1.58% since 2023.
For inquiries
Isabell Rabe
Head of Press and Politics
Phone: 07141/9790-9845
E-mail: presse@mhplus.de
About the SBK:
SBK Siemens-Betriebskrankenkasse is the largest company health insurance fund in Germany and is one of the 20 largest statutory health insurance funds. As an open, nationwide health insurance company, it insures more than one million people and looks after over 100,000 corporate customers in Germany – with around 2000 employees in 86 branches. For more than 100 years, SBK has been personally committed to the interests of its policyholders. It positions itself as a pioneer for genuine quality competition in statutory health insurance. From the SBK’s point of view, the prerequisite for this is more transparency for the insured – about relevant key financial figures, but also about the willingness to perform, advice and service quality of health insurance companies. In the interests of the customer, SBK also combines the best of the personal and digital worlds and is actively driving forward digitalization in the healthcare sector.
For inquiries
Julia Mederle
Corporate Communications Department
Phone: +49 89 62700-363
E-mail: julia.mederle@sbk.org Internet: www.sbk.org
Other News
contextflow & Neologica partner to bring comprehensive chest CT support to radiologists
Vienna, Austria (June 5, 2024) – Neologica, the long-running developer of advanced medical imaging software solutions, and contextflow announce a commercial partnership to bring contextflow’s ADVANCE Chest CT solution to Neologica’s radiology base.
Under the partnership, contextflow’s innovative computer-aided detection support for chest CT will be integrated into Neologica’s LogiPACS. Founded in 2002, Neologica develops a range of products, including a PACS server, DICOM viewer and online patient portal. All of the company’s products are developed in-house for maximum interoperability. By partnering with contextflow, Neologica can offer its users a powerful tool to detect lung cancer, ILD patterns and COPD on chest CT.
contextflow’s core technology is ADVANCE Chest CT, an AI-based medical device software that detects, visualizes and quantifies nodules and lung disease patterns to improve the speed and quality of radiology reporting with consistent, objective information. Its upcoming malignancy scoring feature has been shown to not only detect lung cancer sooner but also to reduce both false positives and false negatives (*Adams, Scott J et al., JACR September 2022).
As Marco Sambin, CEO at Neologica explains, “It’s undeniable that the PACS market is expressing a strong demand for diagnostic decision support solutions through AI. Neologica’s partnership with contextflow is a response to this request within the realm of chest CT imaging. ADVANCE Chest CT is an extremely advanced (CE MDR certified) product for the detection of lung nodules and other lung pathologies. Users of our LogiPACS and RemotEye Viewer will have access to an AI-enhanced workflow with seamless integration into our software modules.”
In addition to increased access to clinical decision support for chest CT, the partnership aims to reduce false positives and patient stress in relation to lung cancer detection via malignancy scoring. Malignancy scoring is a newly released feature that enables a radiologist to compare suspicious nodules to thousands of others with known outcomes in order to indicate the probability that a given nodule is malignant or benign. As contextflow Chief Commercial Officer Marcel Wassink puts it, “Malignancy scoring has been validated in a clinical study to reduce false positive nodule detection by 18% while detecting lung cancer up to one year earlier. We hope this level of certainty helps avoid patient anxiety and reduce unnecessary costs and work for radiologists.”
About contextflow
contextflow is a spin-off of the Medical University of Vienna (MUW) and European research project KHRESMOI, supported by the Technical University of Vienna (TU). Founded by a team of AI and engineering experts in July 2016, the company has a strong interest in bringing state-of-the-art machine learning techniques to the market e.g. improved emphysema detection and lung segmentation. Its computer-aided detection software ADVANCE Chest CT is CE Marked and available for clinical use within Europe under the new MDR.
About Neologica
Neologica is an ISO 9001 and ISO 13485-certified company designing and developing advanced software solutions in the medical imaging field.
With more than 20 years of history and experience, and developing the initial goal of specializing in the DICOM field, today Neologica has a complete range of DICOM-compliant software products in the medical imaging field. This range is composed of software modules that the company has designed and developed in-house from the ground up, covering everything from visualization to archiving, from printing to data exchange. Today, Neologica continues to innovate with original ideas and a strong focus on the quality of its products.
With 5000+ installations across 40+ countries and 5 continents, along with a record of highly satisfied customers, Neologica is now a recognized actor in the medical imaging domain.
The professionalism and skills of its human resources are fundamental values for Neologica; exceeding customers’ expectations with its products is the company’s main objective.
For more information, contact:
Julie Sufana, Chief Marketing Officer, contextflow, email: julie@contextflow.com
Phone: +43 6769201032
Marco Sambin, Chief Executive Officer, Neologica, email: marco.sambin@neologica.it
Phone: +39 019 505314
Other News
contextflow targets early lung cancer detection by augmenting ADVANCE Chest CT with malignancy scoring from RevealDx
Vienna, Austria (02.05.2024) – Chest CT experts contextflow GmbH have released a new version of their comprehensive computer-aided detection support tool, ADVANCE Chest CT. In addition to lung nodule detection, quantification, visualization and classification, the updated software now analyzes nodules for malignancy with the aim of detecting cancer early and reducing unnecessary procedures.
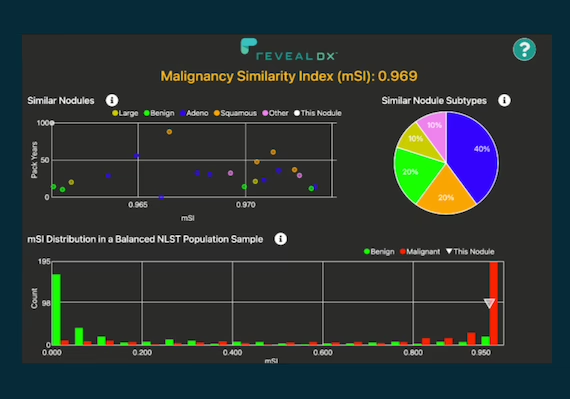
It’s widely known that lung cancer constitutes one of the leading causes of premature death, and thus early detection of cancer is crucial. For that very reason, contextflow has implemented a malignancy Similarity Index (mSI) feature into ADVANCE Chest CT, a clinical decision support tool that aids radiologists in the diagnosis of lung cancer, interstitial lung diseases (ILD) and chronic-obstructive pulmonary disease (COPD).
A malignancy Similarity Index is a value from 0 to 1 that indicates the degree of similarity between a nodule in question and nodules with known outcomes in a reference set. In clinical practice, a high mSI would indicate “upgrading” followup of a nodule as compared to guideline recommendations because there is increased certainty that the nodule in question is malignant. Here, the goal is to detect cancer as early as possible in order to improve patient outcomes.
As contextflow CEO Markus Holzer puts it, “Detecting lung cancer is a challenging and time-consuming task for radiologists. Detection is not straightforward. All too often patients are scheduled for followups months after their initial exam without knowing whether they actually have cancer or not. This is extremely stressful, but thankfully we can start to change that.”
On the flip side, a low mSI score would indicate “downgrading” the nodule with the aim of reducing invasive, unnecessary procedures and patient stress. In a clinical study published in the Journal of the American College of Radiology, use of the RevealDx mSI feature was shown to detect cancer up to one year sooner in approximately 45% of cases while simultaneously reducing false positive detection rates by 18% (Adams, Scott J. et al. JACR September 2022).
As Chris Wood, CEO of RevealDx says, “Our integration with ADVANCE Chest CT simplifies the interpretation of lung nodules. Automatically detected nodules have their mSI scores calculated before the radiologist starts reading the exam, which should save time while providing clinical insight.”
The latest version of contextflow ADVANCE Chest CT also includes a nodule tracking report to visualize and quantify changes in nodules over time. contextflow ADVANCE Chest CT is a CE marked medical device under MDR. For more information, contact sales@contextflow.com or visit contextflow.com.
About contextflow
contextflow is a spin-off of the Medical University of Vienna (MUW) and European research project KHRESMOI, supported by the Technical University of Vienna (TU). Founded by a team of AI and engineering experts in July 2016, the company has a strong interest in bringing state-of-the-art machine learning techniques to the market e.g. improved emphysema detection and lung segmentation. Its computer-aided detection software ADVANCE Chest CT is CE Marked and available for clinical use within Europe under the new MDR. Visit contextflow.com for more information.
About RevealDx
RevealDx developed RevealAI-Lung, the world’s first CADx software for the characterization of lung nodules to receive the CE Mark. RevealAI-Lung has been validated in clinical studies that show improvement in diagnostic precision using our patented methods. Results demonstrate the software can significantly accelerate lung cancer diagnosis and reduce unnecessary procedures. https://reveal-dx.com/
For more information, contact:
Julie Sufana, Chief Marketing Officer, contextflow
Email: julie@contextflow.com
Phone: +43 676 920 1032
Chris Wood, CEO, RevealDx
Email: chris@reveal-dx.com
Phone: +01 425 895 2845
Other News
contextflow gewinnt den Wettbewerb Healthy Hub von vier Krankenkassen: Innovative Lösungen für Frauengesundheit und Früherkennung
DORTMUND, 13.03.2024. Die Gewinnerinnen und Gewinner des Healthy-Hub-Wettbewerbs 2024 wollen die Gesundheit von Frauen mit innovativer Versorgung verbessern. Die verschiedenen Angebote beziehen sich auf unterschiedliche Lebensphasen und Krankheitsbilder – von hybriden Tests gegen HPV-Viren, über die Versorgung bei frauentypischen Krankheiten wie Endometriose, bis hin zu einer innovativen Therapie bei Beschwerden in der Menopause. Menschen mit Lungenerkrankungen sollen in Sachen Früherkennung besser betreut werden. Diese Themen gehen die Siegerteams jeweils mit einer der vier Krankenkassen – BIG direkt gesund, IKK Südwest, mhplus Krankenkasse und SBK Siemens-Betriebskrankenkasse – an. Die Kassen haben den Wettbewerb bereits zum fünften Mal gemeinsam ausgerichtet.
„Im Fokus standen dieses Mal selektivvertragliche Versorgungslösungen, die insbesondere das Gender Health Gap, also die Ungleichheit der Versorgung von Frauen gegenüber Männern, berücksichtigen sollten“, erläutert Dr. Elmar Waldschmitt, Geschäftsführer des Healthy Hub und Vorstandsbeauftragter bei der BIG. Die medizinische Forschung und Versorgung sei leider immer noch zu stark auf Männer fokussiert.
Aus gut 40 Bewerbungen wurden die Gewinnerinnen und Gewinner ausgewählt. Diese sind:
Remi Health, Kassenpartnerin BIG direkt gesund
Remi Health hat eine Früherkennung gegen Gebärmutterhalskrebs entwickelt, bei der sich weibliche Versicherte zuhause auf Humane Papillomviren (HPV) testen können. Bei auffälligem Befund sind eine Online-Beratung und die Terminvereinbarung bei einer Gynäkologin oder einem Gynäkologen vorgesehen. Die digitale Plattform von Remi klärt zudem über die Bedeutung der Vorsorge und Früherkennung auf. „Der niedrigschwellige HPV-Test vereint Heimtests, Telemedizin und Prävention in einem nahtlosen Prozess“, erläutert Marvin Abert, Co-CEO von Remi Health. „Damit möchten wir insbesondere junge Frauen erreichen, die bislang die Krebsvorsorgeuntersuchungen nicht in Anspruch nehmen und keine Immunität durch eine HPV-Impfung besitzen. Der HPV-Selbsttest von Remi Health ist unserer Ansicht nach ein innovativer Lösungsansatz, um die Krebsvorsorge sinnvoll zu ergänzen“, sagt Christiane Heidrich, Teamleiterin Managed Care der BIG direkt gesund.
Femna Health, Kassenpartnerin SBK Siemens-Betriebskrankenkasse
Rund ein Drittel der Frauen im fertilen Alter, also in den fruchtbaren Jahren, leidet unter stark einschränkenden physischen, psychischen und sozialen Belastungen aufgrund von Zyklusbeschwerden. Darunter fallen Erkrankungen wie PMS, Endometriose oder auch Dysmenorrhö. „Die aktuelle Versorgung geht unter anderem aufgrund von mangelnden Therapiemöglichkeiten, langen Wartezeiten und fehlender individueller Betreuung diese Probleme nicht adäquat an. FEMNA hat deshalb ein hybrides Versorgungsmodell entwickelt, das Frauen eine verbesserte, vollumfängliche und sofortige Versorgung ermöglicht“, erklärt Maxie Matthiessen, Gründerin von Femna Health. „Femna Care verbessert Verhaltensmuster und hilft, Folgeerkrankungen zu vermeiden sowie die Lebensqualität betroffener Frauen zu steigern“, sagt Christina Bernards, Teamleiterin Versorgungsmanagement, SBK Siemens-Betriebskrankenkasse. „Für uns ein echtes Herzensthema, denn gerade die Frauengesundheit wird in Medizin und Forschung massiv vernachlässigt und unterfinanziert. Es wird Zeit, dass wir das ändern.“
YoniCare, Kassenpartnerin mhplus Krankenkasse
Mit YoniCare (MICADO HEALTH CARE GmbH) hat der Healthy Hub erstmals ein nicht-digitales Versorgungsprodukt im Portfolio. YoniCare ermöglicht eine Lasertherapie zur Behandlung des genitourinären Syndroms. „Der sinkende Östrogenspiegel in der Menopause führt bei Frauen unter anderem zu Scheidentrockenheit, Veränderungen im Vaginalgewebe sowie der Vaginalschleimhaut und in der Folge zu Beschwerden wie Jucken, Inkontinenz, Infekten und anderen Beschwerden“, so Mandy Wilms von der MICADO HEALTH CARE GmbH. Die Therapie kann das vaginale Epithel revitalisieren, das die Vagina und den Scheidenvorhof auskleidet. Die Beschwerden nehmen ab und die gynäkologische Gesundheit wird wiederhergestellt. „Die Therapie kann eine Hormonersatztherapie überflüssig machen und Wechselwirkungen mit Medikamenten reduzieren“, sagt Fabienne Knaub, Referentin Selektivverträge und Versorgungsanalyse der mhplus Krankenkasse.
contextflow, Kassenpartnerin IKK Südwest
Bei Erkrankungen im Thoraxbereich ist eine Früherkennung wesentlich für den Therapieerfolg. „Wir bieten eine KI-Software, die ergänzende Informationen zur Identifizierung und Interpretation von lungenspezifischen Bildmustern in Scans vom Computertomographen bietet“, so Markus Holzer, CEO und Co-Founder von contextflow. Das ultimative Ziel der Software ist es, Lungenkrebs so früh wie möglich zu erkennen, um Ressourcen des Gesundheitssystems zu sparen und Patientinnen und Patienten vor unnötigen Eingriffen zu schützen. „Die Bildanalyse-KI ermöglicht den befundenden Radiologen eine schnellere und bessere Beurteilung relevanter Bildmuster von Lungenkrebs und respiratorischen Erkrankungen“, sagt Dr. Florian Brandt, Health Innovation Manager der IKK Südwest.
Anwendungsfälle für die Versorgungspraxis entwickeln
Die vier Krankenkassen entwickeln in den nächsten Monaten gemeinsam den Gewinnerteams konkrete Anwendungsfälle, die für den Einsatz in der Gesetzlichen Krankenversicherung (GKV) geeignet sind. „Unser Ziel ist es, dass diese innovativen Versorgungsmethoden in der Versorgungspraxis ankommen“, so Dr. Elmar Waldschmitt. Zudem wird der Kooperationspartner des Healthyhub, die GWQ ServicePlus AG, in die Entwicklung von Anfang an eingebunden.
Über den Healthy Hub
Seit 2018 engagieren sich die vier Krankenkassen BIG direkt gesund, IKK Südwest, mhplus Krankenkasse sowie SBK Siemens-Betriebskrankenkasse mit dem Healthy Hub für die Digitalisierung des Gesundheitswesens. Ziel ist es, innovative Lösungen für eine bessere, integrierte Versorgung zu ermöglichen. Dazu organisieren die Kassen regelmäßig Wettbewerbe für Start-ups. So haben sie bereits 27 Start-ups in die Versorgung gebracht.
Über BIG direkt gesund
Die BundesInnungskrankenkasse Gesundheit – kurz BIG direkt gesund – wurde 1996 in Dortmund gegründet. Die große Idee hinter der BIG: Wir schaffen Raum fürs Menschsein. Gemeint ist damit eine moderne Online-Ausrichtung und empathischer Service, der schnell und lösungsorientiert ist. Die BIG bietet vielseitige Kommunikationswege passend zum jeweiligen Lebensstil ihrer bundesweit rund 510.000 Versicherten. Diese Kundinnen und Kunden erfahren eine wertschätzende und verständliche Beratung per Telefon, Chat, Mail oder Brief. Viele Zusatzleistungen sowie ein attraktives Bonusprogramm sind weitere große Pluspunkte. BIG direkt gesund hat ihren Rechtssitz in Berlin, ihre Hauptverwaltung in Dortmund und einen wichtigen Verwaltungsstandort in Aachen. Die BIG beschäftigt an den operativen Standorten rund 950 Mitarbeiterinnen und Mitarbeiter, in 11 BIGshops wird Beratung vor Ort angeboten.
Für Rückfragen
Bettina Kiwitt
Leiterin Unternehmenskommunikation
Tel.: 0231/5557-1016
E-Mail: bettina.kiwitt@big-direkt.de
Über die IKK Südwest:
Aktuell betreut die IKK Südwest mehr als 635.000 Versicherte und über 90.000 Betriebe in Hessen, Rheinland-Pfalz und im Saarland. Versicherte und Interessenten können auf eine persönliche Betreuung in unseren 21 Kundencentern in der Region vertrauen. Darüber hinaus ist die IKK Südwest an sieben Tagen in der Woche rund um die Uhr über die IKK Service-Hotline 0681/ 3876 1000 oder www.ikk-suedwest.de zu erreichen.
Für Rückfragen
Mathias Gessner
Pressesprecher
Tel.: 0681/3876-1163
E-Mail: presse@ikk-sw.de
Über die mhplus Krankenkasse:
Die mhplus Krankenkasse ist offen für gesetzlich Krankenversicherte. Rund 1.000 Mitarbeitende betreuen deutschlandweit mehr als eine halbe Million Versicherte. Unabhängige Tests belegen hohe Servicestandards und solide Finanzen. Der Zusatzbeitrag der mhplus beträgt seit 2023 stabil 1,58 Prozent.
Für Rückfragen
Isabell Rabe
Leiterin Presse und Politik
Tel.: 07141/9790–9845
E-Mail: presse@mhplus.de
Über die SBK:
Die SBK Siemens-Betriebskrankenkasse ist die größte Betriebskrankenkasse Deutschlands und gehört zu den 20 größten gesetzlichen Krankenkassen. Als geöffnete, bundesweit tätige Krankenkasse versichert sie mehr als eine Million Menschen und betreut über 100.000 Firmenkunden in Deutschland – mit rund 2000 Mitarbeiterinnen und Mitarbeitern in 86 Geschäftsstellen. Seit über 100 Jahren setzt sich die SBK persönlich und engagiert für die Interessen der Versicherten ein. Sie positioniert sich als Vorreiter für einen echten Qualitätswettbewerb in der gesetzlichen Krankenversicherung. Voraussetzung dafür ist aus Sicht der SBK mehr Transparenz für die Versicherten – über relevante Finanzkennzahlen, aber auch über Leistungsbereitschaft, Beratung und Dienstleistungsqualität von Krankenkassen. Im Sinne des Kunden vereint die SBK darüber hinaus das Beste aus persönlicher und digitaler Welt und treibt die Digitalisierung im Gesundheitswesen aktiv voran.
Für Rückfragen
Julia Mederle
Stab Unternehmenskommunikation
Tel.: +49 89 62700-363
E-Mail: julia.mederle@sbk.org Internet: www.sbk.org
Other News
contextflow included in Spanish study on rheumatoid arthritis and ILD diagnosis
The Spanish Society of Rheumatology is currently conducting a research study to explore the prevalence and early diagnosis of interstitial lung disease (ILD) in individuals diagnosed with rheumatoid arthritis (RA). Fifteen rheumatology departments will work on the study together with the radiology departments in Spain in 2024 and 2025, and hereby make use of radiology AI in rheumatology.
This collaboration will address an important healthcare issue: the early detection of ILDs, which tend to go undetected until later stages. This, in turn, negatively impacts patient outcomes, particularly when a patient suffers from cardiovascular diseases.
Rheumatoid arthritis is a systemic autoimmune disease that predominately involves joints, but it can develop into inflammation in lungs, heart, eyes. The expectation is that approximately 30% of rheumatoid arthritis patients may develop diffuse ILDs, underscoring the need for effective screening criteria. Early diagnosis is hard due to the lack of standard. To achieve this goal, the research team has outlined specific criteria for participant selection, and the study aims to recruit over 450 patients across 15 hospital centers. The study results will hopefully help define strategies for early detection of ILD in patients with rheumatoid arthritis.
contextflow ADVANCE Chest CT as the AI solution will deliver automatic quantification regarding the extent of ILD in the study population, enabling detailed examination of the lung parenchyma. Furthermore, the study will compare the interstitial involvement of the lung parenchyma in chest CTs assessed by radiologists and compare them to the results from the automatic detection of ILD-associated patterns by contextflow’s AI software.
While specific lung patterns under assessment remain unclear, the integration of AI-driven analysis promises to enhance accuracy and efficiency of diagnosis.
Radiology AI solution for better diagnosis
This collaborative effort aims to improve early detection and management of ILDs in rheumatoid arthritis patients, potentially leading to better outcomes and quality of life for affected individuals. It is a great example of how radiology AI solution can be used in rheumatology.
Other News
Improving diagnosis for incidental pulmonary embolism (IPE) in the clinical workflow: the role of AI
In July 2023, Erasmus Medical Center’s radiology department kicked off a four-year project focusing on the use of CT to improve diagnosis and treatment outcomes of incidental pulmonary embolism (IPE). The project was made possible through a grant from the NHI (Netherlands Health Institute) and is a collaboration between contextflow and esteemed partners in the Netherlands:
- Erasmus Medical Center, Department of Radiology in Rotterdam
- Erasmus School of Health Policy and Management (ESHPM), Department of Health Technology Assessment in Rotterdam
- Technical University Delft, Department of Imaging Physics in Delft
The project is evolving under the guidance of the dedicated PhD student Erik Kemper at Erasmus University and will explore ways in which machine learning-based technology can be seamlessly blended into workflows to help radiologists and clinicians catch IPEs earlier and more accurately.
Besides an obvious benefit to patients and radiologists (and a seeming benefit to hospitals and the healthcare system at large) the use of AI in clinical practice has never really been explored for IPE. Therefore, the project will look into the impact of the technological advancement of PE detection in various settings with the aim of redefining the landscape of radiology and potentially set new benchmarks in efficiency and patient-centered care as they relate to IPE.
This collaboration shows the power of interdisciplinary cooperation in medical technology innovation. Over the course of the next four years, the involved parties will work on producing results that could be used for setting new standards for radiology and healthcare.
What is incidental pulmonary embolism (IPE) and why use AI to detect it?
Incidental pulmonary embolism is a life-threatening condition that requires prompt diagnosis and treatment. Detecting PE in computed tomography (CT) scans can be challenging, and the project group believes AI can help in improving the accuracy and consistency of IPE detection by analyzing and identifying subtle patterns that may go unnoticed by human observers and by reducing false negatives and false positives.
The interpretation of medical imaging can be time-consuming, especially in busy healthcare settings. AI algorithms can rapidly analyze images and assist radiologists in the detection of IPE, potentially reducing the time required for diagnosis.
By providing consistent and reproducible results, AI algorithms can also help reduce inter-observer variability and ensure that the same criteria are applied to every case. This standardization can lead to more reliable diagnoses, enabling better patient management and facilitating research and quality improvement initiatives.
Other News
Blackford and contextflow Announce Commercial Partnership to Bring Comprehensive Chest CT Detection Software to Healthcare Providers
Edinburgh, Scotland (November 16th, 2023) – Blackford, the pioneering strategic AI platform and solutions provider, and contextflow today announced a commercial partnership to bring contextflow’s ADVANCE Chest CT solution to healthcare professionals.
Under the partnership, contextflow’s innovative technology will be integrated with Blackford’s advanced enterprise AI platform. Blackford provides healthcare professionals access to an extensive portfolio of medical AI solutions designed to drive clinical efficiency and improve patient outcomes. By integrating contextflow’s advanced detection technology into the Blackford platform, Blackford can offer healthcare providers a powerful tool for detecting ILD, COPD and lung cancer on chest CTs.
“Blackford exists to improve the lives of patients and populations – we can do this by providing tailored AI solutions to healthcare providers around the world to help enhance therapy selection and treatment optimisation”, said Ben Panter, CEO of Blackford. “We are delighted to partner with contextflow to add their advanced tools for lung disease detection, quantification and monitoring of disease progression to our AI portfolio.”
contextflow’s CE and UKCA marked technology, ADVANCE Chest CT, offers radiologists comprehensive computer-aided detection support for lung cancer, ILD, and COPD patients. The software detects, visualizes and quantifies nodules and lung disease patterns to enhance the speed and quality of radiology reports. Its upcoming malignancy scoring feature has been shown to not only detect lung cancer sooner but also to reduce both false positives and false negatives (*Adams, Scott J et al., JACR September 2022).
As contextflow’s Chief Commercial Officer Marcel Wassink puts it, “Successful implementation of lung cancer screening programs will require the use of assistive AI to help with earlier detection and manage the workloads. We also understand that lung cancer is only one of many findings relevant to the patient’s wellbeing, and thus we are proud to offer comprehensive support for chest CT that goes beyond cancer to include ILD, COPD, and in the near future, incidental pulmonary embolism. Our partnership with Blackford will accelerate the adoption of this much-needed AI, increasing its accessibility to radiologists and patients alike.”
About Blackford
Blackford are pioneers in the radiology AI space, with over a decade of experience working in partnership with leading hospitals and ground-breaking technology providers. We operate as a strategic AI partner, providing access to a tried-and-tested core platform, tailored services, and a portfolio of 100+ applications to help healthcare providers unlock the value of AI and improve patient outcomes.
Our collaboration and recent arms-length acquisition by Bayer ensures that our customers and partners have the support and long-term security needed to underpin successful AI strategies.
To learn more about Blackford’s tailored approach to AI solutions visit www.blackfordanalysis.com.
About contextflow
contextflow is a spin-off of the Medical University of Vienna (MUW) and European research project KHRESMOI, supported by the Technical University of Vienna (TU). Founded by a team of AI and engineering experts in July 2016, the company has a strong interest in bringing state-of-the-art machine learning techniques to the market e.g. improved emphysema detection and lung segmentation. Its computer-aided detection software ADVANCE Chest CT is CE Marked and available for clinical use within Europe under the new MDR. Visit contextflow.com for more information.
Other News
Always in the picture thanks to AI

Evangelisches Klinikum Niederrhein introduces contextflow ADVANCE Chest CT in the Pulmonology Department
Lung diseases are among the most common as well as most diverse health problems worldwide. They require precise diagnoses and effective treatment strategies. In this context, artificial intelligence (AI) opens up a promising avenue for detecting a wide variety of disease conditions in affected patients as early as possible. Fanar Othman, head physician at the Clinic for Pulmonary and Bronchial Medicine at Johanniter Hospital Oberhausen, has also discovered the possibilities of deep learning-based technology for himself. He uses the CE certified software contextflow ADVANCE Chest CT to ensure that even when there is a lot to do, the pulmonologist no longer misses anything.
As part of the Lower Rhine Evangelical Hospital and Bethesda Hospital network, the department not only cares for around 3,000 patients a year in its own hospital, but also provides consultative care for three other sites in the western Ruhr region, including Dinslaken and Duisburg. As a former stronghold of the coal and steel industry, the region is also known as the “coal pot”. Particularly among the older generation, the doctors still see many patients whose health was severely affected by their work in the former mines, blast furnaces and factories. As a result, a not insignificant proportion of the medical care provided locally is for occupational lung diseases such as pneumoconiosis, silicosis, asbestosis and, unfortunately, the resulting late effects such as cancer and pleural mesothelioma.
So there is a lot to do for the total of five pulmonologists under the direction of Fanar Othman. “We have a large catchment area and, simply because of the size of our association, we get to see a large number of rare pathologies in addition to the usual clinical findings,” says the chief physician. “In these cases, it can already become a challenge to make the correct diagnosis and initiate appropriate therapy.” In this context, a single disease may be associated with multiple radiological patterns. Precise characterization is often laborious and examiner-dependent.
Quick access to relevant knowledge
Since last year, contextflow’s AI solution has been providing a remedy for this problem. It takes over the sifting and provision of information from CT examinations that are relevant for diagnostics. The recognition software detects even small changes in the lung parenchyma and relates them to specific diseases. For nodules, it can even show progression. The resulting findings report is generated automatically and is available directly in the PACS viewer within a few minutes. In this way, the tool saves the diagnostician from having to work through thousands of image slices every day, and at the same time, prevents anything important from being overlooked.
Using an AI system in his department is new territory for Fanar Othman. He was made aware of ADVANCE Chest CT by his physician colleague, the head of radiology, Prof. Dr. Jörg Michael Neuerburg, who has already been using the software successfully for some time. “From the beginning, I liked how affable and user-friendly the application was,” Othman recalls. “You have to take care of practically nothing. The findings generated by the AI are prepared in a simple and clearly understandable way, so you can adopt the results without time-consuming cross-checking. There is not enough time for anything else in daily practice. Everything has to be done in a jiffy.”
Progress controls at the push of a button
When the opportunity arose to take part in a product training course initiated by contextflow, the pulmonologist jumped at the chance. During the online training, he discovered that the software can do a lot more that is valuable for his work: “For example, the AI is able to compare different series of images taken at different points in time. This makes it possible to assess the size development of nodules, which is very important for determining further therapeutics.”
In addition to calculating the diameter in a plane, the system also applies 3D volumetric analysis to evaluate the total mass of a pulmonary nodule. The volumetric measurement method is becoming increasingly important because it offers a more accurate assessment of malignancy risk, or tumor grade, compared to linear measurement, and also helps to better monitor response to therapy – especially when it comes to determining tumor doubling time. This refers to the fact that in most malignant lesions, volume increases first, followed by size.
From the pattern of findings to differential diagnosis
The software solution is also used for texture analysis, e.g. for characterizing parenchymal changes such as ground-glass opacities, reticular pattern or honeycombing. In this context, the distribution of the changes in the lung allows decisive conclusions to be drawn about the underlying clinical picture. However, differential diagnosis is a difficult and complex task due to the sheer number of existing lung pathologies. In addition, it is often the small but subtle differences that matter. Even experienced experts sometimes reach their limits here. “Sometimes it’s difficult to decide with subtle changes in the lower lobe: is this an emphysema bullae or honeycombing? The AI can differentiate such structures incredibly well,” Fanar Othman is pleased to report.
What the Oberhausen head physician also likes is that the structural parenchymal changes can be displayed in percentage form with the help of ADVANCE Chest CT: “When a check-up is due, you can’t always tell with the naked eye whether it has improved after therapy or not. If the response is not that great, it’s helpful to know by what percentage it ultimately got better. A lot of patients ask us explicitly about that, too.” So such clear feedback can have a positive effect on doctor-patient communication.
Overall, the expert is very pleased with how AI has been able to reduce the workload in his department over the past year while increasing diagnostic accuracy. He says his team is also enthusiastic and has already asked him – or rather the AI – for advice in one or two tricky cases. Othman is not worried that a machine could one day outstrip him: “I see it as an opportunity – especially in view of the fact that there is a shortage of staff anyway. AI is therefore a helpful support in the diagnostic process that makes a lot of things easier. In the end, it is still us who bring it all together with the laboratory values, clinical data and samples and come to a decision. That remains the fine art and continues to be the physician’s task.”
Other News
Stets im Bild dank KI
Evangelisches Klinikum Niederrhein führt contextflow ADVANCE Chest CT in der Pneumologie ein
Lungenerkrankungen gehören weltweit zu den am häufigsten auftretenden sowie vielfältigsten Gesundheitsproblemen. Sie erfordern präzise Diagnosen und effektive Behandlungsstrategien. In diesem Zusammenhang eröffnet Künstliche Intelligenz (KI) einen vielversprechenden Weg, um verschiedenste Krankheitsbilder bei betroffenen Patienten so früh wie möglich zu erkennen. Auch Fanar Othman, Chefarzt der Klinik für Lungen- und Bronchialheilkunde am Johanniter Krankenhaus Oberhausen, hat die Möglichkeiten von Deep-Learning-basierter Technologie für sich entdeckt. Im Bereich der computertomographischen Bildgebung nutzt er das CE-zertifizierte KI-Programm contextflow ADVANCE Chest CT. Selbst wenn viel zu tun ist, entgeht dem Pneumologen so nichts mehr.
Als Teil des Verbunds Evangelisches Klinikum Niederrhein und BETHESDA Krankenhaus Duisburg betreut die Abteilung nicht nur jährlich um die 3.000 Patienten im eigenen Haus, sondern übernimmt darüber hinaus noch die konsiliarische Mitbetreuung von drei weiteren Standorten im westlichen Ruhrgebiet, darunter Dinslaken und Duisburg. Als ehemalige Hochburg der Kohle- und Stahlindustrie ist die Region auch als „Kohlenpott“ bekannt. Besonders in der älteren Generation sehen die Ärzte bis heute viele Patienten, denen ihre Arbeit in den früheren Bergwerken, Hochöfen und Fabriken massiv auf die Gesundheit geschlagen ist. Daher entfällt ein nicht unwesentlicher Teil der medizinischen Versorgung vor Ort auf berufsbedingte Lungenerkrankungen wie Staublunge (Pneumokoniose), Silikosen, Asbestosen und leider auch die daraus resultierenden Spätfolgen wie Krebs und Pleuramesotheliome.
Viel zu tun also für die insgesamt neun Ärzte unter der Leitung von Fanar Othman. „Wir haben ein großes Einzugsgebiet und bekommen allein aufgrund der Größe unseres Verbundes neben den gängigen Krankheitsbildern auch eine Vielzahl seltener Pathologien zu Gesicht, die nicht so alltäglich sind“, so der Chefarzt. „In diesen Fällen kann es schon zur Herausforderung werden, die richtige Diagnose zu stellen und eine entsprechende Therapie einzuleiten.“ Dabei kann eine einzelne Erkrankung mit mehreren radiologischen Mustern verbunden sein. Eine genaue Charakterisierung ist oft mühsam und untersucherabhängig.
Schneller Zugriff auf relevantes Wissen
Seit letztem Jahr schafft die KI-Lösung von contextflow Abhilfe bei diesem Problem. Sie übernimmt das Sichten und Bereitstellen von für die Diagnostik relevanten Informationen aus CT-Untersuchungen. Dabei spürt die Erkennungssoftware selbst kleine Veränderungen im Lungenparenchym auf und stellt sie in Zusammenhang mit bestimmten Erkrankungen und deren Verlauf. Der daraus resultierende Befundbericht wird automatisch generiert und steht innerhalb weniger Minuten direkt im PACS-Viewer zur Verfügung. Auf diese Weise erspart das Tool dem Befunder, sich täglich durch Tausende von Schichtbildaufnahmen zu arbeiten und verhindert gleichzeitig, dass wichtige Erkenntnisse übersehen werden.
Der Einsatz eines KI-Systems in seiner Abteilung ist Neuland für Fanar Othman. Aufmerksam gemacht wurde er auf ADVANCE Chest CT von seinem Arztkollegen, dem Chefarzt der Radiologie, Prof. Dr. Jörg Michael Neuerburg, der die Software bereits seit längerer Zeit erfolgreich nutzt. „Mir gefiel von Anfang an, wie umgänglich und benutzerfreundlich die Anwendung ist“, erinnert sich Othman. „Man muss sich praktisch um nichts kümmern. Die von der KI erstellten Befunde sind einfach und klar verständlich aufbereitet, sodass man die Ergebnisse ohne aufwendige Gegenprüfung übernehmen kann. Für alles andere bleibt in der täglichen Praxis auch gar nicht die Zeit. Da muss alles zack, zack gehen.“
Verlaufskontrollen auf Knopfdruck
Als sich die Gelegenheit bot, an einer von contextflow initiierten Produktschulung teilzunehmen, zögerte der Pneumologe nicht lang und ergriff die Chance. Während des Onlinetrainings stellte er fest, dass die Software noch einiges mehr kann, was für seine Arbeit von Wert ist: „Zum Beispiel ist die KI in der Lage, unterschiedliche Serien von Aufnahmen, die zu verschiedenen Zeitpunkten gemacht wurden, miteinander zu vergleichen. Dies ermöglicht es, die Größenentwicklung von Rundherden zu beurteilen, was sehr wichtig für das weitere therapeutische Vorgehen ist.“
Neben der Berechnung des Durchmessers in einer Ebene wendet das System auch die 3D-Volumenanalyse an, um die Gesamtmasse einer Lungenläsion zu bewerten. Die volumetrische Messmethode gewinnt zunehmend an Bedeutung, da sie im Vergleich zur linearen Messung eine genauere Einschätzung des Malignitätsrisikos bzw. des Tumorgrads bietet und außerdem dabei hilft, die Reaktion auf eine Therapie besser zu überwachen – insbesondere, wenn es darum geht, die Tumorverdopplungszeit festzustellen. Damit ist gemeint, dass bei den meisten bösartigen Läsionen zuerst das Volumen zunimmt, dann die Größe.
Vom Befundmuster zur Differentialdiagnose
Des Weiteren kommt die Softwarelösung auch bei der Texturanalyse zum Einsatz, z. B. bei der Charakterisierung von Parenchymveränderungen wie Milchglastrübungen, netzartigen retikulären Mustern oder Honigwabenbildung. Dabei lässt die Verteilung der Veränderungen in der Lunge entscheidende Rückschlüsse auf das zugrunde liegende Krankheitsbild zu. Dennoch gestaltet sich die Differentialdiagnose allein aufgrund der schieren Masse an existierenden Lungenpathologien als schwierige und komplexe Aufgabe. Hinzukommt, dass es häufig die kleinen, aber feinen Unterschiede sind, auf die es ankommt. Selbst erfahrene Experten stoßen hier teilweise an ihre Grenzen. „Manchmal ist es schwierig, bei subtilen Veränderungen im Unterlappen zu entscheiden: Ist das ein Emphysembullae oder Honigwabenmuster? Solche Strukturen kann die KI unglaublich gut differenzieren“, freut sich Fanar Othman.
Was dem Oberhausener Chefarzt außerdem gefällt, ist, dass sich die strukturellen Parenchymveränderungen mithilfe von ADVANCE Chest CT in prozentualer Form darstellen lassen: „Wenn eine Kontrolluntersuchung ansteht, kann man nicht immer mit bloßem Auge erkennen, ob es nach der Therapie besser geworden ist oder nicht. Wenn das Ansprechen nicht so großartig ausfällt, ist es hilfreich zu wissen, um wie viel Prozent es letztendlich besser geworden ist. Viele Patienten fragen uns auch explizit danach.“ So ein eindeutiges Feedback kann sich also positiv auf die Arzt-Patienten-Kommunikation auswirken.
Insgesamt zeigt sich der Experte sehr zufrieden damit, wie die KI die Arbeitslast in seiner Abteilung im letzten Jahr reduzieren konnte und gleichzeitig die diagnostische Genauigkeit erhöht hat. Auch sein Team sei begeistert und habe ihn – oder besser gesagt die KI – in dem ein oder anderen kniffeligen Fall schon um Rat gefragt. Dass eine Maschine ihm eines Tages den Rang ablaufen könnte, darüber macht sich Othman keine Sorgen: „Ich empfinde es als Chance – gerade auch vor dem Hintergrund, dass ohnehin Personalmangel herrscht. Die KI stellt daher eine hilfreiche Unterstützung bei der Befundung dar, die vieles erleichtert. Am Ende sind es immer noch wir, die das Ganze mit den Laborwerten, klinischen Daten und Proben zusammenführen und zu einer Entscheidung kommen. Das bleibt die hohe Kunst und weiterhin Aufgabe des Arztes.“